This article is for educational purposes only. Always consult your healthcare provider before starting, stopping, or changing GLP-1 medication.
With GLP-1 medications dominating health headlines, a parallel wave of online content has begun conflating GLP-1 with its molecular cousin, GLP-2. Some websites market "GLP-2 activators" or "GLP-1/GLP-2 protocols" for weight loss. Wellness influencers have started discussing GLP-2 supplements. And patients occasionally ask their providers whether GLP-2 should be part of their treatment plan.
The short answer: GLP-2 is not a weight loss hormone, and GLP-2 activation is not a recognized treatment for obesity. But understanding why reveals something genuinely interesting about gut biology — and helps you identify misleading health claims when you encounter them.
What Are GLP-1 and GLP-2?
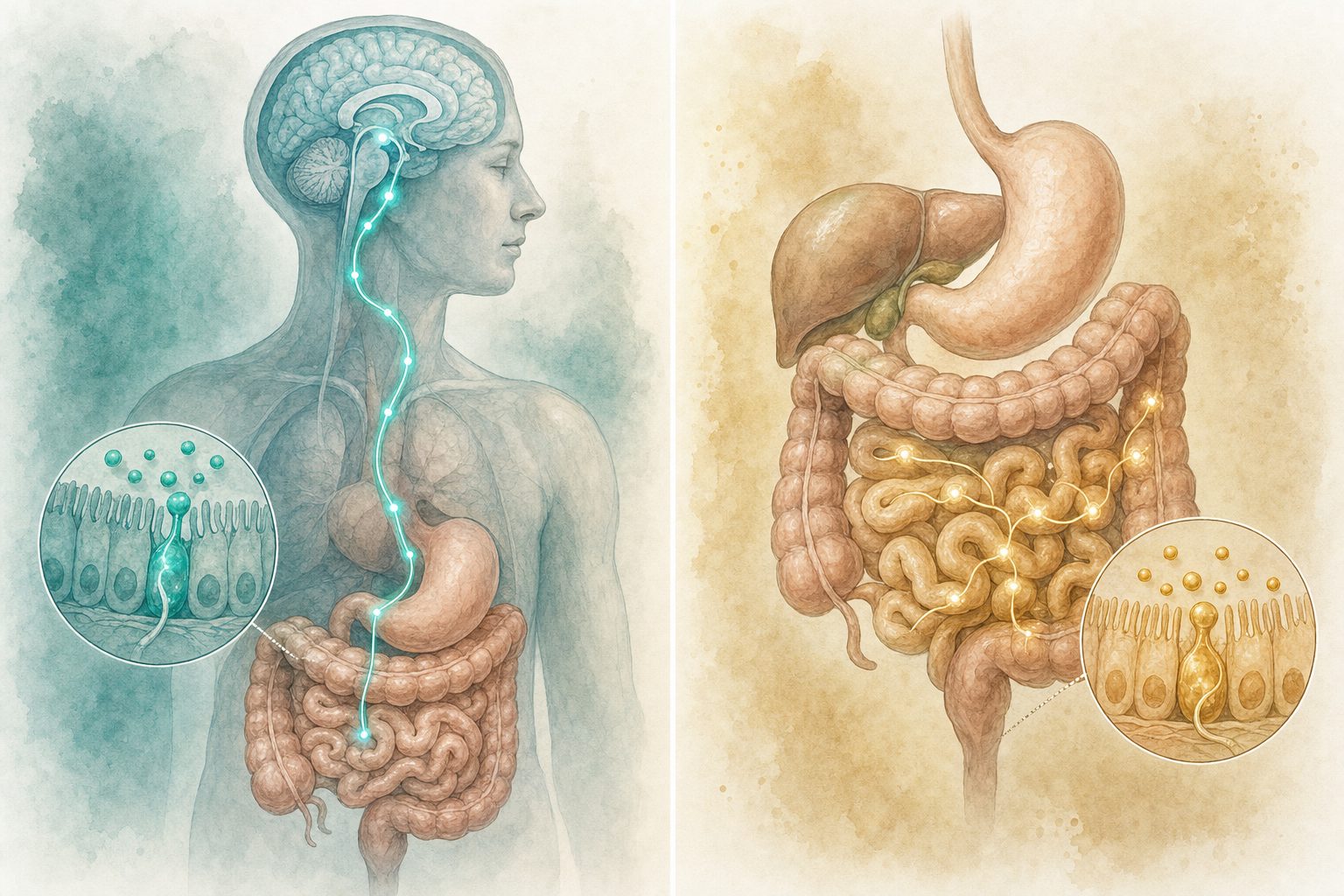
Both GLP-1 and GLP-2 are peptide hormones produced by the same specialized intestinal cells — the L-cells of the small intestine and colon. Both are products of the same precursor protein, proglucagon, and both are released in response to nutrients in the gut. That's where the similarity largely ends.
They act on completely different receptors, in different tissues, with entirely different physiological functions.
GLP-1: The Appetite and Insulin Hormone
GLP-1 (glucagon-like peptide-1) is:
- An incretin hormone — it stimulates the pancreas to release insulin after eating (in a glucose-dependent manner, meaning only when blood sugar is elevated)
- A satiety signal — GLP-1 receptors in the hypothalamus and brainstem reduce appetite and food intake
- A gastric motility regulator — slows the rate at which food empties from the stomach, extending the feeling of fullness
- A glucagon suppressor — reduces liver glucose output, a key driver of fasting hyperglycemia in type 2 diabetes
The drugs that mimic GLP-1 (semaglutide, tirzepatide, liraglutide) work because GLP-1 does all of these things and more. They're agonists — they bind GLP-1 receptors and activate them just like the natural hormone, but last much longer in the body.
GLP-2: The Intestinal Growth Hormone
GLP-2 (glucagon-like peptide-2) is a fundamentally different animal. Its receptor (GLP-2R) is found primarily in the intestinal epithelium, enteric nervous system, and gut submucosal layers — not in the hypothalamus, not in the pancreas.
GLP-2's primary physiological role is intestinal trophism — stimulating the growth, maintenance, and repair of the gut lining. Specifically, it:
- Increases villus height in the small intestine (the finger-like projections that absorb nutrients)
- Reduces intestinal permeability ("leaky gut," in common parlance)
- Reduces intestinal inflammation
- Increases nutrient absorption efficiency by promoting a healthy gut mucosal surface
- Reduces intestinal cell death (apoptosis)
The only FDA-approved GLP-2 receptor agonist as of 2026 is teduglutide (Gattex), which is used to treat short bowel syndrome — a serious condition where patients have had large portions of their small intestine surgically removed and cannot absorb adequate nutrition. In this context, GLP-2 helps the remaining intestine compensate by growing a more functional mucosal surface.
Teduglutide's FDA approval is specifically for "short bowel syndrome in patients who are dependent on parenteral support." It is given as a daily subcutaneous injection and its risks include accelerating the growth of intestinal neoplasms (colorectal cancer screening is required before and during use).
Why "GLP-2 for Weight Loss" Is a Myth
GLP-2 does not suppress appetite. It does not slow gastric emptying in a clinically meaningful way. It does not signal the hypothalamus to reduce food intake. Activating GLP-2 receptors stimulates gut growth — which if anything increases nutrient absorption efficiency.
The claim that GLP-2 activation promotes weight loss has no clinical evidence base. A search of published randomized controlled trials yields no evidence that GLP-2 agonism produces weight loss in humans with obesity.
Some wellness content confuses GLP-2's role in reducing gut inflammation with a broad health benefit that somehow extends to metabolism. While gut health and metabolic health are interrelated areas of active research, GLP-2 activation specifically is not a weight management intervention.
Why does this matter? Because some supplement marketers promote products as "activating GLP-1 and GLP-2" together, implying dual benefits. In reality: - No supplement has demonstrated meaningful GLP-1 receptor agonism equivalent to pharmaceutical GLP-1 medications - Adding GLP-2 activation language does not enhance any weight loss claim — it's a category error, mixing an appetite hormone with a gut growth hormone - Supplements promoting "GLP-2 activation" for weight loss are making claims that are not supported by human clinical evidence
Where GLP-2 Research Is Actually Going
There is legitimate scientific interest in GLP-2 — just not for obesity. Areas of active investigation include:
Short Bowel Syndrome and Intestinal Failure
Teduglutide (Gattex) is an established treatment here, and research continues on long-acting formulations and expanded populations (e.g., pediatric patients, Crohn's disease-associated bowel resection).
Intestinal Barrier Function and Metabolic Disease
Some research groups are investigating whether reduced intestinal permeability (a GLP-2 effect) might contribute to better metabolic outcomes in metabolic syndrome or type 2 diabetes — not by suppressing appetite, but by reducing translocation of bacterial endotoxins from the gut into the bloodstream, which drives systemic inflammation. This is mechanistically interesting but far from a clinical application for weight management. Key work from Cani et al. in Diabetes established the gut permeability–metabolic disease link, but GLP-2 as a treatment for metabolic disease remains unproven.
Combination Therapy: Dapiglutide and GLP-1/GLP-2 Dual Agonism
One genuinely novel research direction involves dapiglutide, a dual GLP-1/GLP-2 receptor agonist being developed by Zealand Pharma (the same company partnered with Boehringer Ingelheim on survodutide). The rationale is not primarily weight loss — it's for short bowel syndrome, where adding GLP-1 activity might help with glycemic control alongside the GLP-2 intestinal growth effect.
A Phase 1/2 trial of dapiglutide is underway. This is intestinal medicine, not obesity medicine — and it illustrates how even the most advanced GLP-2-related science doesn't frame GLP-2 as a weight loss target.
The Proglucagon Connection: Why the Confusion Happens
Both GLP-1 and GLP-2 are cleaved from the same precursor molecule, proglucagon. The same gene (GCG) produces proglucagon, which is then processed differently in different tissues:
- In the pancreas: Proglucagon → glucagon (the blood-sugar-raising hormone)
- In the intestinal L-cells: Proglucagon → GLP-1, GLP-2, and oxyntomodulin
- In the brain: Similar processing to the intestine
This shared origin explains why some research papers reference the "proglucagon-derived peptides" as a family — and why casual reading can blur the functional distinctions between them. But sharing a molecular precursor doesn't make them interchangeable any more than having the same manufacturer makes a heart medication and a blood pressure drug equivalent.
What to Say When You See "GLP-2 for Weight Loss"
If you encounter content claiming GLP-2 activation is a weight loss strategy:
- Ask for evidence. Is there a randomized controlled trial in humans with obesity showing GLP-2 agonism reduces body weight? There isn't.
- Check the FDA status. The only approved GLP-2 drug (teduglutide/Gattex) is for short bowel syndrome, not weight management.
- Note the mechanism. GLP-2 receptors are not in appetite-regulating brain regions. GLP-2 grows intestinal tissue; it does not reduce hunger.
- Consider who benefits from the confusion. Supplement companies frequently leverage scientific-sounding terminology to suggest pharmaceutical-like effects. GLP-2 language in a supplement context is almost always a marketing tactic, not a clinical claim.
Independent Analysis: Why the GLP-1 vs. GLP-2 Distinction Actually Matters Clinically
Three mechanistic observations that explain why GLP-1 and GLP-2 produce such different clinical outcomes despite sharing a common precursor:
1. The tissue distribution of receptors explains everything
GLP-1 receptors are expressed in the hypothalamus, brainstem, pancreatic beta cells, cardiac muscle, and gut enteroendocrine cells — a distribution that explains why GLP-1 agonists simultaneously suppress appetite, stimulate insulin secretion, slow gastric emptying, and have cardiovascular effects. GLP-2 receptors are expressed almost exclusively in intestinal epithelial cells (enterocytes), enteric neurons, and subepithelial myofibroblasts. The GLP-2 receptor biology review in Frontiers in Endocrinology identifies GLP-2's primary function as intestinotrophic — promoting growth and repair of the intestinal lining. This is why teduglutide (Gattex), the GLP-2 agonist approved for short bowel syndrome, increases intestinal absorptive capacity rather than reducing appetite. The two receptors do not cross-activate at physiological concentrations.
2. The shared precursor creates genuine pharmacological complexity in the next generation of drugs
Both GLP-1 and GLP-2 are post-translational processing products of the same gene — proglucagon — but are processed differently depending on tissue type. In the pancreas, proglucagon is processed into glucagon (which raises blood glucose). In intestinal L-cells, it is processed into GLP-1, GLP-2, and oxyntomodulin. This means any drug that targets proglucagon-derived pathways broadly — or that incorporates both GLP-1 and GLP-2 activity — must navigate opposing effects. Oxyntomodulin, which activates both GLP-1 and GLP-2 receptors, has been studied as a potential obesity treatment, but its dual receptor activity requires careful dose management to avoid unintended intestinal proliferation alongside desired appetite suppression. The oxyntomodulin pharmacology literature shows this is an active but unresolved research area, not a clinically available approach.
3. The confusion in patient-facing content has a specific origin
A notable pattern in GLP-1 patient communities is confusion between GLP-1 and "GLP" broadly — partly because drug names like "GLP-1 agonist" are sometimes shortened to just "GLP," and partly because some wellness marketing uses "gut peptide" language loosely to describe various supplements. There are no commercially available GLP-2 supplements, and no GLP-2 receptor agonist has any obesity indication — approved or investigational as of 2026. When a product claims to "activate GLP pathways" without specifying GLP-1 specifically, the claim is either non-specific or, in some cases, is borrowing GLP-1's clinical credibility for a product with no mechanism connecting it to GLP-1 receptor activity. Patients researching this area benefit from distinguishing FDA-approved GLP-1 receptor agonists from products using adjacent terminology.
What this means for patients on GLP-1 medications
The GLP-1/GLP-2 distinction is primarily educational for most GLP-1 users — there is no practical interaction or clinical overlap to manage. Where it becomes practically relevant is in evaluating marketing claims for supplements or compounded peptides. If a product cites "incretin" or "GLP" effects without specifying GLP-1 receptor agonism backed by published data, that is a signal to look more carefully. See our peptide therapy overview for context on distinguishing FDA-approved medications from the broader research-peptide market.
Frequently Asked Questions
What is GLP-2 and what is it used for?
GLP-2 (glucagon-like peptide-2) is a gut hormone that promotes growth and repair of the intestinal lining. The FDA-approved GLP-2 receptor agonist is teduglutide (Gattex), used to treat short bowel syndrome — a condition where the intestine cannot absorb enough nutrients. GLP-2 has no role in weight loss or diabetes management.
Can GLP-2 agonists cause weight loss?
No. GLP-2 receptor agonists act on intestinal epithelium to increase mucosal surface area and absorption. They have no appetite-suppressing effect and no relevant central nervous system activity. In short bowel syndrome, they are used to improve nutrient absorption — the opposite goal from weight management.
Why are GLP-1 and GLP-2 grouped together if they do such different things?
Both are derived from the same precursor protein, proglucagon, processed in intestinal L-cells. They are numbered sequentially because they were discovered and characterized in the same research program in the 1980s. Beyond the naming convention and shared precursor, they function through distinct receptors in entirely different tissues and should not be grouped clinically.
What is the difference between GLP-1, GIP, and glucagon — the three proglucagon-related hormones?
GLP-1 (glucagon-like peptide-1) stimulates insulin secretion and reduces appetite. GIP (glucose-dependent insulinotropic peptide) also stimulates insulin and is the second receptor targeted by tirzepatide. Glucagon raises blood glucose by stimulating glycogen breakdown in the liver. Retatrutide targets all three — GLP-1, GIP, and glucagon — which is why it is called a triple agonist. These three hormones have overlapping but distinct effects that make combination targeting a complex pharmacological challenge.
Is teduglutide (Gattex) related to Ozempic or Wegovy?
Only in that both are incretin-family drugs derived from proglucagon-related peptides. Teduglutide is a GLP-2 analog and acts on GLP-2 receptors in the intestinal wall. Semaglutide (Ozempic, Wegovy) is a GLP-1 analog and acts on GLP-1 receptors in the brain, pancreas, and gut. They share no clinical application overlap and are approved for entirely different conditions.
Are there any supplements that actually activate GLP-1 receptors?
No approved dietary supplement activates GLP-1 receptors with the potency or mechanism of semaglutide or tirzepatide. Some foods and nutrients (berberine, fiber, certain fatty acids) may modestly stimulate endogenous GLP-1 secretion from intestinal L-cells, but this is a physiological response affecting circulating GLP-1 levels by a small amount — not receptor agonism. Products claiming to mimic GLP-1 medication effects via supplementation are not supported by equivalent clinical evidence.
What is oxyntomodulin and why does it matter for this comparison?
Oxyntomodulin is another proglucagon-derived peptide that activates both GLP-1 and GLP-2 receptors. It has been studied as a potential appetite suppressant, but its dual GLP-1/GLP-2 activity means it also has intestinotrophic effects. No oxyntomodulin-based drug has reached FDA approval. It represents the pharmacological space between pure GLP-1 agonists and pure GLP-2 agonists — an interesting research target, not a current clinical option.
Sources
- Drucker DJ. "The biology of incretin hormones." Cell Metabolism, 2006. https://www.cell.com/cell-metabolism/fulltext/S1550-4131(06)00078-6
- Holst JJ. "The physiology of glucagon-like peptide 1." Physiological Reviews, 2007. https://journals.physiology.org/doi/full/10.1152/physrev.00034.2006
- FDA. "Gattex (teduglutide) Prescribing Information." https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/203441s011lbl.pdf
- Cani PD, et al. "Metabolic endotoxemia initiates obesity and insulin resistance." Diabetes, 2007. https://diabetes.diabetesjournals.org/content/56/7/1761
- Zealand Pharma. "Dapiglutide Pipeline Information." https://www.zealandpharma.com/pipeline/dapiglutide/
- Brubaker PL, Drucker DJ. "Minireview: Glucagon-Like Peptides Regulate Cell Proliferation and Apoptosis in the Pancreas, Gut, and Central Nervous System." Endocrinology, 2004. https://academic.oup.com/endo/article/145/6/2653/2499660